Henry was a 12 yr-old-boy with a history of poor attention, impulse control issues, peer relation difficulties and non compliant behavior. His parents and grandmother reported that, “Henry came out difficult.”
He was the product of prolonged labor and was born “blue” but no concerns from the physician were noted. Colic, sleep problems, constipation, picky eating, and sensory issues were present in early childhood. Henry was easily upset and had difficulties getting along with his older sister and younger brother, as well as kids in school.
At age four, his preschool teacher expressed concerns about Henry’s behavior and recommended that they speak to their pediatrician about Attention-Deficit Hyperactivity Disorder (ADHD). After a visit to the pediatrician and completion of the Vanderbilt Rating Scales, Henry was diagnosed with ADHD and prescribed Concerta for ADHD.
Henry’s behavior improved for the remainder of preschool with noticeable improvement in focus and seat work. By the end of the summer and just before kindergarten, Henry’s side effects from the medication, low appetite, caused him to not eat to the point that he was lethargic and losing weight. At the pediatrician’s suggestion, they added PediaSure, which helped Henry gain weight but worsened his constipation (he was only eliminating a couple of times a week).
In Kindergarten, an IEP plan was put in place under the Other Health Impairment (OHI) category. His impulsiveness and mood was getting in the way of transitioning, work completion, and peer relationships. Although Henry was bright with an above average IQ of 117, his work production was poor. Throughout the years, a variety of school-based interventions were put into place. They all seemed to alleviate the problem to some degree but nothing ever seemed to really work.
Henry switched
ADHD medications, which resulted in ups and downs behaviorally. His parents tried to get him to eat healthy but Henry would hoard cookies and soda and other carb foods. They would find wrappers in his room and he only stopped when the whole family gave it up. They noticed a positive shift when they cleaned up his diet and switched to soda and 100 percent juice.
Henry participated in private social skills groups in later elementary school and into middle school. Peer and sibling relations were hard for Henry because he was so impulsive that he didn’t slow down enough to connect with others. He was also easily angered, which wore out other kids. He did best socially in highly structured activities and when his parents were close by to intervene.
In middle school, coupled with hormone changes, Henry’s mood worsened, so his pediatrician recommended a consult with a psychiatrist. Risperdal, an antipsychotic medication to address his mood, was added but his diagnosis of ADHD did not change. Henry became very flat and gained twenty pounds in a short period of time. His parents became concerned and sought help from me at this point.
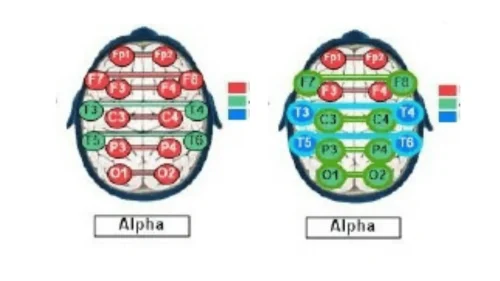
Henry’s QEEG Brain Map reflected a high amount of Delta and High Beta brainwave activity wrapped around his frontal lobes, which is often seen in birth trauma and other head injury. Henry also had high levels of Alpha brainwaves, which is common in those with mood regulation issues and disorders. He had excessive brain communication in Alpha. Overall, his brain reflected exactly what his behavior looked like, high levels of dysregulation.
%20.png)