The Growing Crisis and "The Regulation Gap"
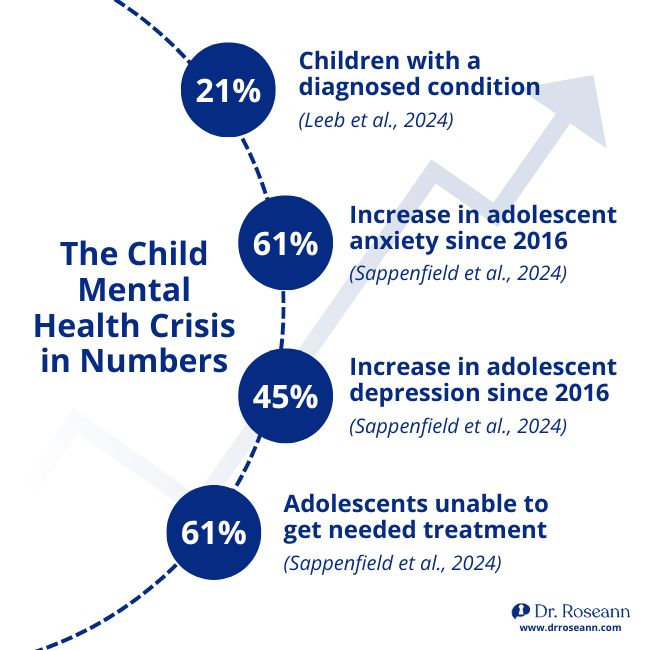
The numbers are impossible to ignore. According to the Centers for Disease Control and Prevention, nearly 1 in 5 children ages 3 to 17 — approximately 21% — had ever been diagnosed with a mental, emotional, or behavioral health condition as of 2021 (Leeb et al., 2024). Among adolescents ages 12 to 17, 20% reported symptoms of anxiety and 18% reported symptoms of depression in the past two weeks (Centers for Disease Control and Prevention, 2025). In 2023, more than 5.3 million adolescents — 20.3% of all adolescents — carried a current, diagnosed mental or behavioral health condition (Sappenfield et al., 2024).
| The Scope of the Crisis |
Statistic |
| Overall Prevalence |
Nearly 1 in 5 children ages 3–17 (21%) had a diagnosed mental, emotional, or behavioral condition in 2021 (Leeb et al., 2024). |
| Adolescent Anxiety |
20% of adolescents ages 12–17 reported symptoms of anxiety in the past two weeks (Centers for Disease Control and Prevention, 2025). |
| Adolescent Depression |
18% of adolescents ages 12–17 reported symptoms of depression in the past two weeks (Centers for Disease Control and Prevention, 2025). |
| Growth Rate |
Between 2016 and 2023, diagnosed anxiety rose by 61%, and depression by 45% (Sappenfield et al., 2024). |
| Treatment Gap |
61% of adolescents who needed treatment reported difficulty getting it (Sappenfield et al., 2024). |
Furthermore, data from 2021-2023 show that over 42% of high school students experienced persistent feelings of sadness or hopelessness during the past year (Verlenden et al., 2024), and older children (ages 12-17) were significantly more likely to have received mental health treatment compared to younger children (Zablotsky & Ng, 2023). These statistics represent real children — children who are struggling to get through a school day, who melt down over small frustrations, who cannot sleep, who avoid food, who rage at their parents, who shut down and disappear into screens. They are not bad kids. They are
dysregulated kids.The Regulation Gap
The core of this crisis is
The Regulation Gap. Modern childhood places immense demands on a child's executive functioning — academic pressure, social media navigation, complex transitions. Yet, at the same time, the environmental
drivers of dysregulation (screen time, sleep disruption, poor nutrition, sensory overload) are depleting the nervous system's capacity to handle those demands.
We are asking children to perform high-level cognitive tasks with a nervous system that lacks the capacity to support them.
The crisis is compounded by a treatment gap. While 61% of adolescents with a current diagnosis who needed treatment reported difficulty getting it (Sappenfield et al., 2024), the more urgent problem is that even when treatment is received, the underlying nervous system dysregulation is rarely addressed. Children receive diagnoses, medications, and therapy, yet the meltdowns continue. The anxiety persists. The behavior escalates.
This is not a failure of the children. It is a failure of the model.
Why Behavior-First Models Miss the Mark
For decades, the dominant approach to child behavior has been compliance-based: set clear expectations, deliver consistent consequences, use reward systems, and correct misbehavior promptly. These approaches are not without value. But they share a critical flaw — they assume the child is regulated enough to respond to them.
When a child is in a stress response state, they are not capable of the cognitive processing that behavior-first interventions require. Consequences do not teach regulation. Reward charts do not build nervous system capacity. Lectures about choices do not reach a brain that is in survival mode. In fact, trauma and emotional dysregulation can directly interfere with the development of emotion regulation and interpersonal skills, leaving the child vulnerable to being emotionally overwhelmed by everyday stressors (Paulus, Ohmann, Möhler, Plener, & Popow, 2021).
The same limitation applies to clinical treatment. Cognitive Behavioral Therapy (CBT), Dialectical Behavior Therapy (DBT), and Exposure and Response Prevention (ERP) are widely used evidence-based approaches. Each of them relies on the child's ability to identify thoughts, challenge beliefs, tolerate discomfort, and apply learned skills. These are executive functioning tasks. And executive functioning collapses under stress (Zelazo, Blair, & Willoughby, 2016).
"Chronic stress and anxiety, often due to family, school, or health issues, is one of the biggest risk factors for executive dysfunction throughout the life span, particularly in children, for whom the executive functions that help us to manage stress have not yet matured." (Calderon, 2020)
This is why so many parents report the same frustrating pattern: their child goes to therapy, seems to understand the concepts, but cannot use the tools when it matters most. As Keeshin, Bryant, and Gargaro (2021) note, exploring the presence of trauma reminders is pertinent, because trauma reminders are often innocuous, everyday events that trigger behavioral outbursts in emotionally dysregulated youth. The child is not resistant. The child is dysregulated. And a dysregulated brain cannot access the prefrontal cortex skills that therapy requires.
The problem is not the therapy. The problem is the missing foundation: regulation.
The Neuroscience of Dysregulation
To understand why regulation must come first, we need to understand what happens in the brain when a child is stressed.
The autonomic nervous system (ANS) is the body's threat-detection and response system. According to Polyvagal Theory, developed by Dr. Stephen Porges, the nervous system operates in a hierarchy of responses (Caffrey, 2023):
- Ventral Vagal (Safe): Supports social engagement, learning, and connection.
- Sympathetic (Threat): Activates the fight-or-flight response.
- Dorsal Vagal (Extreme Threat): Triggers shutdown, collapse, or dissociation.
Critically, this threat detection process, which Porges calls "neuroception," is involuntary (Caffrey, 2023). The child is not choosing to go into fight-or-flight. Their nervous system is responding automatically to perceived danger. This is why telling a dysregulated child to "calm down" or "use your words" is physiologically ineffective — the part of the brain that processes language and makes rational choices is not fully online.
The prefrontal cortex (PFC) is the brain's executive control center. It is responsible for impulse control, emotional regulation, decision-making, working memory, and flexible thinking. The PFC is highly interconnected with the amygdala, which drives the stress response. When the amygdala signals threat, it effectively hijacks the PFC (Zelazo, Blair, & Willoughby, 2016). As McEwen (2007) explains, the brain is the organ that interprets experiences as threatening or non-threatening, and the acute and chronic effects of stressful experiences directly influence how it responds.
The stress response itself is a cascade. Any disruption to homeostasis activates the sympathetic-adrenal-medullary (SAM) axis and the hypothalamic-pituitary-adrenal (HPA) axis, releasing adrenaline and cortisol (Chu et al., 2024). The SAM axis produces the rapid fight-or-flight response. The HPA axis produces a slower cortisol release that peaks 15 to 25 minutes after stress induction and can take an hour to return to baseline. This means that even after the triggering event is over, the child's body is still flooded with stress hormones — making regulation, learning, and behavior change physiologically impossible in the short term.
This is not a character issue. It is a brain-state issue.
QEEG Evidence — What 10,000+ Brain Maps Reveal
One of the most powerful aspects of the Regulation First framework is that it is grounded in objective, measurable data. Quantitative Electroencephalography (QEEG) is a tool that maps brainwave activity across the cortex, providing a window into how the brain is actually functioning — not how we assume it is functioning.
Over more than 30 years of clinical practice, Dr. Roseann Capanna-Hodge has conducted and reviewed more than 10,000 QEEGs. What these brain maps reveal, consistently and across thousands of children and adolescents, is that the behaviors we label as ADHD, anxiety, depression, defiance, and emotional dysregulation are associated with measurable, identifiable patterns of nervous system dysregulation.

Research confirms what these clinical observations show. Elevated beta wave activity in the temporal lobes — particularly at the T3 and T4 sites — is significantly associated with anxiety, fear, insecurity, and panic. In one study, 89.6% of individuals with elevated temporal beta waves reported anxiety, and 84.4% reported fear, compared to rates of 8.4% and 4.4% in control groups (Ribas et al., 2018). An excess alpha wave pattern is strongly associated with the co-occurrence of internalizing disorders such as anxiety, depression, and emotional dysregulation (Kopańska & Trojniak, 2025).
These patterns are not random. They are the brain's response to chronic stress, trauma, and dysregulation. They are visible. They are measurable. And they explain why behavior-first interventions fail — because the brain driving the behavior is not in a state that can respond to them.
The QEEG data also reveals the impact of environmental stressors. Stress has been demonstrated to affect higher cognitive activities including decision-making and working memory, with EEG frequency domain analysis showing that the brain's oscillatory activity changes in distinct patterns under stress (Yan et al., 2024). When a child's brain is chronically operating in a stress state, these changes become entrenched — creating the patterns of dysregulation that parents and clinicians observe as persistent behavior problems.
Environmental Drivers of Dysregulation
Children today are navigating a world that their nervous systems were not designed for. The cumulative load of modern stressors — academic pressure, social comparison, sensory overload, disrupted sleep, nutritional deficits, and above all, screen exposure — is overwhelming developing regulatory systems.
Compounded Stressors and Bidirectional Co-Dysregulation
Dysregulation rarely occurs in isolation; it is driven by the compounding effect of multiple stressors. Chronic stress and adverse childhood experiences create an "allostatic load"—cumulative wear and tear on the nervous system that progressively impairs emotional regulation and physiological health (Finlay et al., 2022). For children, this means that academic pressures, sensory overload, and social challenges do not act independently; they compound to overwhelm the nervous system's capacity.
Crucially, this compounded stress is bidirectional between parent and child. A child's internalizing and externalizing problems act as chronic stressors that increase parental emotional dysregulation, while parental dysregulation simultaneously impairs the child's ability to learn and practice emotion regulation (Wang et al., 2025). When a dysregulated child interacts with a stressed, dysregulated parent, the result is co-dysregulation—a vicious cycle where each nervous system escalates the other. This bidirectional effect demonstrates why treating the child in isolation often fails; the family system itself must be regulated.
Sleep and Emotional Regulation
Sleep is one of the most powerful regulators of the nervous system, and it is one of the most disrupted. Disturbances of the circadian rhythm and sleep are directly associated with affect dysregulation, increased substance use, and risky behaviors in adolescents (Paulus, Ohmann, Möhler, Plener, & Popow, 2021). A child who is not sleeping well is a child whose nervous system cannot recover from the stressors of the day — creating a cycle of dysregulation that compounds over time.
Sensory Overload and Nutrition
Many children with dysregulation also struggle with sensory processing challenges that affect eating, learning, and daily functioning. Sensory defensiveness, particularly in the tactile domain, is associated with food avoidance and the kind of mealtime battles that exhaust families (Fonseca et al., 2024). Furthermore, neurodevelopmental disorders like Autism Spectrum Disorder (ASD) and Attention Deficit Hyperactivity Disorder (ADHD) are highly comorbid with these sensory-based feeding issues (Fonseca et al., 2024). These are not picky eaters making bad choices. These are children whose nervous systems are overwhelmed by sensory input.
Device Dysregulation®
Perhaps the most significant and underappreciated driver of dysregulation in today's children is screen exposure. Digital devices activate dopamine and reward pathways, providing instant emotional relief that substitutes for — and ultimately undermines — the development of internal regulation capacity (Pető et al., 2024).
The research is clear: screen time at a younger age is negatively associated with later self-regulation and executive function (Pető et al., 2024). Adolescents with more than two hours of screen time per day show increased symptoms of anxiety and depression and decreased wellbeing (Khan, Lee, & Horwood, 2022). Girls are particularly susceptible to developing socioemotional problems with greater screen use, while boys are more likely to increase screen use when facing socioemotional challenges (Vasconcellos et al., 2025).
Most critically, when parents use devices to manage a child's emotions — a pattern called Parental Digital Emotion Regulation — they inadvertently prevent the child from developing the internal regulatory mechanisms they need. For children with immature self-regulatory skills, dependence on devices to regulate emotions directly interferes with the development of those skills (Pető et al., 2024). The result is a child who cannot tolerate frustration, cannot transition off screens without a meltdown, and cannot self-soothe without external stimulation.
This is Device Dysregulation® — and it is one of the defining challenges of raising children in the digital age.
The Science of Co-Regulation
Here is the truth that changes everything: children cannot regulate themselves. Not because they are choosing not to, but because the neurological capacity for self-regulation is built gradually, through thousands of
co-regulation experiences with a calm, attuned adult.
Co-regulation is not a parenting technique. It is a biological necessity.
Research on parent-child heart rate variability (HRV) synchrony demonstrates that parents strongly shape their children's emotional experience and regulation capacity through autonomic processes (De Witte, Sütterlin, Braet, & Mueller, 2016). The vagus nerve — the primary pathway of the parasympathetic nervous system — plays a central role in this process. Higher vagally mediated resting HRV in adults corresponds to greater ability to regulate, and this capacity is transmitted to children through the quality of the co-regulatory relationship (De Witte et al., 2016).
According to Polyvagal Theory, the sympathetic nervous system's fight-or-flight responses predominate when the parasympathetic nervous system's regulatory functions fail (Beauchaine, Gatzke-Kopp, & Mead, 2007). When a parent is dysregulated — anxious, frustrated, reactive — their nervous system signals threat. The child's nervous system picks up that signal and escalates. This is not a metaphor. It is neurophysiology.
The inverse is equally true. When a parent is regulated — calm, grounded, present — their nervous system signals safety. The child's nervous system begins to co-regulate with the parent's. Behavior improves not because of what the parent said or did, but because of the physiological state the parent brought to the interaction.
Research on parenting behaviors and HRV confirms this. Consistent, emotionally attuned parenting is associated with higher resting HRV in adolescents, which in turn supports greater emotional regulation capacity (Graham, Scott, & Weems, 2017). Parents who are emotionally well-regulated themselves facilitate their children's ability to regulate emotional arousal in response to environmental changes (Graham et al., 2017).
The most powerful parenting intervention is not a new strategy or a better consequence system. It is the parent's own nervous system regulation.The Development of Self-Regulation and Executive Function
Self-regulation does not arrive fully formed. It is grown — slowly, through years of co-regulation, scaffolded practice, and neurological development.
The prefrontal cortex, which houses executive functioning skills, does not fully mature until the mid-20s. This is not a flaw in children's design. It is a biological reality that has profound implications for how we parent and how we treat. Executive function refers to the cognitive processes that enable individuals to manage and regulate their thoughts, actions, and emotions, including planning, attention control, working memory, problem-solving, and task switching (Jensen, 2024). Most models of executive functioning include working memory, attention, task shifting, and response inhibition as key components of executive control (McLean, 2017). These skills are crucial for goal-directed behavior — and they are precisely the skills that collapse under stress.
Neurobiological evidence shows that Adverse Childhood Experiences (ACEs) can significantly impair the structure and function of the prefrontal cortex, affecting cognitive control and strategic thinking (Jensen, 2024). Trauma exposure influences all three core EF components — inhibition, working memory, and cognitive flexibility — making it harder for children who have experienced adversity to regulate, learn, and behave in the ways we expect (Jensen, 2024).
The medial prefrontal cortex and anterior cingulate cortex modulate the amygdala's response to threat. When these areas are underactive — as they are under chronic stress — the amygdala is disinhibited, producing the emotional reactivity, hypervigilance, and behavioral dysregulation that characterize so many of the children seen in clinical practice (Lanius, Frewen, Vermetten, & Yehuda, 2010).
The practical implication is this: when a child cannot use their coping skills, it is not because they are choosing not to. It is because the neurological infrastructure for those skills is temporarily or chronically offline. The answer is not more skills training. The answer is nervous system regulation first.
The Regulation First® Framework
Regulation First Parenting® is a neuroscience-informed framework that establishes nervous system stabilization as the non-negotiable foundation of effective parenting and mental health treatment. It is built on a clear, evidence-based sequence:
1. Regulate
The adult stabilizes their own nervous system first. A dysregulated adult cannot co-regulate a dysregulated child. The adult's calm is the intervention.
2. Connect
Once the adult is regulated, they create safety and connection for the child. This is the co-regulation step — the biological bridge that allows the child's nervous system to shift from threat to safety. Connection is not permissiveness. It is the neurological prerequisite for learning.
3. Correct
Once the child's nervous system is stable enough to access their prefrontal cortex, boundaries, expectations, and accountability can be effectively delivered. Correction delivered in a regulated state is absorbed. Correction delivered in a dysregulated state is escalation.
Without regulation, nothing works. Not consequences. Not therapy. Not medication. Not rewards. Not lectures. Regulation is not one tool among many. It is the foundation upon which every other tool depends.
The Regulation First® framework does not abandon structure, boundaries, or accountability. It sequences them correctly — so they can actually work.
The Paradigm Shift: Before and After Regulation First®
To understand the transformative power of this framework, we must look at how it changes the fundamental response to a dysregulated child.
| The Old Paradigm (Behavior-First) |
The New Paradigm (Regulation First®) |
| Focuses on compliance: "How do I get my child to stop this behavior?" |
Focuses on capacity: "How do I support my child's nervous system so they can regulate?" |
| Assumes intention: Views meltdowns and defiance as choices or manipulation. |
Recognizes physiology: Views meltdowns as an involuntary stress response (fight/flight). |
| Reacts with consequences: Punishes the behavior, which often increases the child's stress load. |
Responds with co-regulation: The adult regulates themselves first to anchor the child's nervous system. |
| Relies on cognitive skills: Demands the child "use their words" or "think about their choices" while dysregulated. |
Relies on neurobiology: Understands the prefrontal cortex is offline and waits for regulation before correcting. |
| Creates exhaustion: Parents and clinicians burn out trying to enforce boundaries on a dysregulated brain. |
Builds resilience: Slowly grows the child's neurological capacity for self-regulation over time. |
The Cost of Inaction
We can no longer afford to treat nervous system dysregulation as a behavioral issue. The cost of continuing with behavior-first and medication-first models is profound.
- The Human Cost: Children who remain chronically dysregulated are at significantly higher risk for long-term anxiety, depression, substance abuse, and academic failure. They spend their formative years in survival mode rather than learning mode.
- The Family Cost: Parents of dysregulated children experience severe burnout, marital strain, and chronic stress. The family ecosystem becomes organized around crisis management rather than connection.
- The Systemic Cost: Schools are overwhelmed by behavioral disruptions that traditional discipline cannot fix. The mental health system is backlogged with children who are receiving therapies they cannot neurologically access.
Addressing the Regulation Gap is not just a clinical preference; it is a public health imperative. If we do not build nervous system capacity first, the investments we make in education and mental health will continue to yield diminishing returns.
Implications for Schools, Clinicians, and Policy
The adoption of Regulation First® principles has transformative implications across every system that touches children's lives.
| Setting |
The Regulation First® Approach |
| Schools |
Learning requires regulation. A child who is dysregulated cannot encode new information, access working memory, or engage in the flexible thinking that academic learning demands. Regulation breaks — brief, structured opportunities for nervous system reset — improve executive functioning and academic engagement. Trauma-informed education frameworks that prioritize safety and co-regulation create the neurological conditions for learning. Schools that build dysregulation-informed practices see reductions in discipline referrals, improved attendance, and better academic outcomes.
|
| Clinicians |
Therapy outcomes depend on nervous system readiness. Before introducing cognitive tools, clinicians must assess and address the child's regulatory state. This means integrating nervous system regulation strategies — breathwork, movement, sensory tools, neurofeedback — as foundational components of treatment, not afterthoughts. It means understanding that a child who "doesn't use the tools" is not resistant; they are dysregulated. And it means recognizing that the therapeutic relationship itself is a co-regulation experience.
|
| Policy |
The youth mental health crisis demands regulation-based frameworks at the policy level. This means funding for dysregulation-informed training in schools and clinical settings, investment in QEEG and neurofeedback research, and policy frameworks that recognize nervous system regulation as a public health priority. The current system treats symptoms. A regulation-informed system addresses root causes.
|
The Path Forward — CALMS Protocol® Certification
The science is clear. The need is urgent. What is required now is a standardized, scalable pathway for implementation.
The CALMS Dysregulation Protocol® is that pathway. Developed by Dr. Roseann Capanna-Hodge, the CALMS Dysregulation Protocol® is a comprehensive, science-based training framework designed to equip parents, educators, and clinicians with the knowledge and tools to implement Regulation First® principles across all settings.
The protocol provides a practical, usable roadmap for adults to stabilize a child's nervous system:
CALMS Dysregulation Protocol®
- C - Co-regulate first: Before addressing behavior, the adult must anchor their own nervous system and bring calm to the interaction. Co-regulation is the biological bridge to the child's self-regulation.
- A - Avoid personalizing: Recognize that the child's dysregulated behavior is a stress response, not an intentional attack. This neurophysiological reframing prevents adult escalation.
- L - Look for root causes: Identify the environmental, sensory, or physiological stressors (such as sleep deficits or Device Dysregulation®) that are driving the nervous system into fight-or-flight.
- M - Model coping strategies: Demonstrate regulated behavior and healthy stress management in real-time, providing the child with a visible template for nervous system recovery.
- S - Support and reinforce: Build long-term regulation capacity through consistent boundaries, connection, and proactive nervous system support.
Through the CALMS Protocol® Certification, practitioners are trained to:
- Understand the neuroscience of dysregulation and the stress response
- Assess nervous system state before any behavioral or cognitive intervention
- Apply the C.A.L.M.S. Dysregulation Protocol® to stabilize the child's nervous system
- Build regulation capacity over time through consistent, dysregulation-informed practice
- Create environments — at home, in school, and in clinical settings — that support nervous system health
The goal is not simply to train individuals. It is to build dysregulation-informed systems — schools, clinical practices, and families that operate from a shared understanding that regulation comes first.
By standardizing this framework and making it accessible at scale, we can change the trajectory of children's mental health. We can reduce the rates of anxiety, depression, and behavioral disorders that are devastating a generation. We can give parents the tools they actually need. We can give clinicians a foundation that makes their work more effective. And we can give children what they deserve: a nervous system that is supported, not overwhelmed.
The missing piece in parenting and mental health treatment is regulation. Regulation First® is the answer.
About Dr. Roseann Capanna-Hodge
Dr. Roseann Capanna-Hodge, Ed.D., LPC, BCN is a pediatric mental health expert, licensed professional counselor, and Board Certified in Neurofeedback with more than 30 years of clinical experience. She is the founder of Regulation First Parenting® and the creator of the CALMS Protocol®. Dr. Roseann has conducted and reviewed more than 10,000 QEEGs and is the author of The Dysregulated Kid: The Parenting Playbook for Helping Your Child Find Calm in a Chaotic World. She is the host of the Dysregulated Kids podcast and a leading voice in the movement to make nervous system regulation the foundation of parenting and mental health care.
Learn more at www.drroseann.com
Resources and Further Reading
For professionals, educators, and parents seeking to implement the Regulation First® framework or deepen their understanding of nervous system regulation, the following resources provide actionable, science-backed guidance:
| Resource |
Description |
Link |
| Regulation First Parenting®: The Complete Guide |
A comprehensive breakdown of the Regulate. Connect. Correct. framework and how to apply it during dysregulation.
|
drroseann.com/post/regulation-first-parenting-complete-guide
|
| The Dysregulated Kid (Book) |
Dr. Roseann's official parenting playbook for helping children find calm in a chaotic world.
|
drroseann.com/post/the-dysregulated-kid-book
|
| Dysregulated Kids Podcast |
A top 1% global podcast offering weekly strategies on emotional dysregulation, ADHD, and anxiety through a nervous system lens.
|
drroseann.com/podcast
|
| CALMS Protocol® Certification |
Parent, CE/CME professional, and organizational certification training in the CALMS Dysregulation Protocol® — the science-based framework for implementing nervous system regulation principles across all settings.
|
drroseann.com/calms
|
References
Beauchaine, T. P., Gatzke-Kopp, L., & Mead, H. K. (2007). Polyvagal Theory and developmental psychopathology: Emotion dysregulation and conduct problems from preschool to adolescence. Biological Psychology, 74(2), 174–184. https://doi.org/10.1016/j.biopsycho.2005.08.008
Caffrey, C. (2023). Polyvagal theory. EBSCO Research Starters. EBSCO Information Services. https://www.ebsco.com/research-starters/health-and-medicine/polyvagal-theory
Calderon, J. (2020, December 16). Executive function in children: Why it matters and how to help. Harvard Health Blog. https://www.health.harvard.edu/blog/executive-function-in-children-why-it-matters-and-how-to-help-202012162348
Centers for Disease Control and Prevention. (2025, June 5). Data and statistics on children's mental health. U.S. Department of Health and Human Services. https://www.cdc.gov/children-mental-health/data-research/index.html
Centers for Disease Control and Prevention. (2024). Youth Risk Behavior Survey Data Summary & Trends Report: 2013–2023. https://www.cdc.gov/yrbs/dstr/
Chu, B., Marwaha, K., Sanvictores, T., Awosika, A. O., & Ayers, D. (2024). Physiology, stress reaction. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK541120/
De Witte, N. A. J., Sütterlin, S., Braet, C., & Mueller, S. C. (2016). Getting to the heart of emotion regulation in youth: The role of interoceptive sensitivity, heart rate variability, and parental psychopathology. PLoS ONE, 11(10), e0164615. https://doi.org/10.1371/journal.pone.0164615
Finlay, S., et al. (2022). Adverse childhood experiences and allostatic load. Neuroscience & Biobehavioral Reviews. https://doi.org/10.1016/j.neubiorev.2022.104734
Fonseca, N. K. O., Curtarelli, V. D., Bertoletti, J., et al. (2024). Avoidant restrictive food intake disorder: Recent advances in neurobiology and treatment. Journal of Eating Disorders, 12, 74. https://doi.org/10.1186/s40337-024-01021-z
Graham, R. A., Scott, B. G., & Weems, C. F. (2017). Parenting behaviors, parent heart rate variability, and their associations with adolescent heart rate variability. Journal of Youth and Adolescence, 46(5), 1089–1103. https://doi.org/10.1007/s10964-016-0616-x
Jensen, J. (2024). Trauma and executive function: Discovering and developing academic motivation interventions for adolescents in residential mental health treatment [Master's capstone project, Hamline University]. DigitalCommons@Hamline. https://digitalcommons.hamline.edu/cgi/viewcontent.cgi?article=2025&context=hse_cp
Keeshin, B. R., Bryant, B. J., & Gargaro, E. R. (2021). Emotional dysregulation: A trauma-informed approach. Child and Adolescent Psychiatric Clinics of North America, 30(2), 375–387. https://doi.org/10.1016/j.chc.2020.10.007
Khan, A., Lee, E.-Y., & Horwood, S. (2022). Adolescent screen time: Associations with school stress and school satisfaction across 38 countries. European Journal of Pediatrics, 181, 2273–2281. https://doi.org/10.1007/s00431-022-04420-z
Kopańska, M., & Trojniak, J. (2025). From aberrant brainwaves to altered plasticity: A review of QEEG biomarkers and neurofeedback in the neurobiological landscape of ADHD. Cells, 14(17), 1339. https://doi.org/10.3390/cells14171339
Lanius, R. A., Frewen, P. A., Vermetten, E., & Yehuda, R. (2010). Fear conditioning and early life vulnerabilities: Two distinct pathways of emotional dysregulation and brain dysfunction in PTSD. European Journal of Psychotraumatology, 1. https://doi.org/10.3402/ejpt.v1i0.5467
Leeb, R. T., Danielson, M. L., Claussen, A. H., Robinson, L. R., Lebrun-Harris, L. A., Ghandour, R., et al. (2024). Trends in mental, behavioral, and developmental disorders among children and adolescents in the US, 2016–2021. Preventing Chronic Disease, 21, Article 240142. https://doi.org/10.5888/pcd21.240142
McEwen, B. S. (2007). Physiology and neurobiology of stress and adaptation: Central role of the brain. Physiological Reviews, 87(3), 873–904. https://doi.org/10.1152/physrev.00041.2006
McLean, S. (2017). Developmental differences in children who have experienced adversity: Difficulty with executive functioning. Child Family Community Australia, Australian Institute of Family Studies. https://aifs.gov.au/resources/practice-guides/developmental-differences-children-who-have-experienced-adversity-guide-no3
Paulus, F. W., Ohmann, S., Möhler, E., Plener, P., & Popow, C. (2021). Emotional dysregulation in children and adolescents with psychiatric disorders: A narrative review. Frontiers in Psychiatry, 12, 628252. https://doi.org/10.3389/fpsyt.2021.628252
Pető, A., Fitzpatrick, C., Lévesque, D., Gergely, A., Bognár, Z., Kotsis, K., Barrett, T., Herrmann, E., & Konok, V. (2024). Cure for tantrums? Longitudinal associations between parental digital emotion regulation and children's self-regulatory skills. Frontiers in Child and Adolescent Psychiatry, 3, Article 1276154. https://doi.org/10.3389/frcha.2024.1276154
Ribas, V. R., Ribas, R. G., Nóbrega, J. A., da Nóbrega, M. V., Espécie, J. A. A., Calafange, M. T., Calafange, C. O. M., & Martins, H. A. L. (2018). Pattern of anxiety, insecurity, fear, panic and/or phobia observed by quantitative electroencephalography (QEEG). Dementia & Neuropsychologia, 12(3), 264–271. https://doi.org/10.1590/1980-57642018dn12-030007
Sappenfield, O., Alberto, C., Minnaert, J., Donney, J., Lebrun-Harris, L., & Ghandour, R. (2024). Adolescent mental and behavioral health, 2023 (Data Brief). U.S. Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Bureau. https://mchb.hrsa.gov/sites/default/files/mchb/data-research/nsch-data-brief-adolescent-mental-behavioral-health-2023.pdf
Vasconcellos, R. P., Sanders, T., Lonsdale, C., Parker, P., Conigrave, J., Tang, S., del Pozo Cruz, B., Biddle, S. J. H., Taylor, R., Innes-Hughes, C., Salmela-Aro, K., Vasconcellos, D., Wilhite, K., Tremaine, E., Booker, B., & Noetel, M. (2025). Electronic screen use and children's socioemotional problems: A systematic review and meta-analysis of longitudinal studies. Psychological Bulletin, 151(5), 513–543. https://doi.org/10.1037/bul0000468
Verlenden, J. V., Fodeman, A., Wilkins, N., Everett Jones, S., Moore, S., Cornett, K., Sims, V., Saelee, R., & Brener, N. D. (2024). Mental health and suicide risk among high school students and protective factors — Youth Risk Behavior Survey, United States, 2023. Morbidity and Mortality Weekly Report (MMWR) Supplement, 73(4), 79–86. https://www.cdc.gov/mmwr/volumes/73/su/su7304a9.htm
Wang, X., et al. (2025). Bidirectional longitudinal relationships between parents' dysregulation, children's emotion regulation and children's internalizing problem. Children and Youth Services Review, 170, 108169. https://doi.org/10.1016/j.childyouth.2025.108169
Yan, B., Wang, Y., Yang, Y., Wu, D., Sun, K., & Xiao, W. (2024). EEG evidence of acute stress enhancing inhibition control by increasing attention. Brain Sciences, 14(10), 1013. https://doi.org/10.3390/brainsci14101013
Zelazo, P. D., Blair, C. B., & Willoughby, M. T. (2016). Executive function: Implications for education (NCER 2017-2000). National Center for Education Research, Institute of Education Sciences, U.S. Department of Education. https://ies.ed.gov/ncer/pubs/20172000/pdf/20172000.pdf
Zablotsky, B., & Ng, A. E. (2023). Mental health treatment among children aged 5–17 years: United States, 2021 (NCHS Data Brief No. 472). National Center for Health Statistics. https://doi.org/10.15620/cdc:128144
Disclaimer: This article is not intended to give health advice and it is recommended to consult with a physician before beginning any new wellness regime. *The effectiveness of diagnosis and treatment vary by patient and condition. Dr. Roseann Capanna-Hodge, LLC does not guarantee certain results.
© Roseann-Capanna-Hodge 2026